Frequently asked questions, find the answers to your questions here.
Breast health and screening FAQs
It is recommended from the age of 40, unless indicated earlier.
Early detection greatly increases the chances for survival and greatly decreases the chances of a mastectomy being necessary for treatment.
Increased media coverage of cases of younger women with celebrity status being diagnosed with breast cancer contributed to the perception that there has been a marked increase in the occurrence of breast cancer among younger women.
There is indeed more breast cancer in younger women, but the increase is rather small and most breast cancer patients in South Africa and abroad have typically been, and still are, women between the ages of 50 and 70.
What is true however is that breast cancer is often missed in younger women as they are often not included in screening programmes. A cancer is therefore usually detected at later stages (when a palpable lump is already present).
It is worthwhile consulting with a specialist about when you should start screening and whether genetic testing could be of value if, as a younger woman, you have close relatives that have cancer.
There are rare forms of breast cancer (inflammatory breast cancer and Paget’s disease of the nipple for example) that can only be diagnosed by doing a clinical examination. These cancers usually cannot be seen by doing a mammogram and/or ultrasound. 5-10% of breast cancers can only be seen on a mammogram in the form of calcifications which do not always show up on ultrasound.
Conversely, about 5-10 % of breast cancers do not image on mammography as they appear like the other normal structures of the breast, but then can be seen on ultrasound.
By doing all three examinations in one visit we can correlate all findings and are thus better able to diagnose a cancer if it is present.
Most important uses of ultrasound in breast imaging are:
- As a primary screening tool for women under the age of 40, who do not yet require a mammogram.
- Cyst vs. solid characterization of clinically occult mammographically detected or palpable breast masses.
- Evaluation of asymmetric tissue on mammogram.
- Evaluation of palpable masses in women who are pregnant, breastfeeding or under 40 years of age.
- Guide for interventional procedures (cyst aspiration, preoperative localization, fine needle aspiration and core biopsy).
The bulk of all mammography performed in South Africa is for screening purposes. The accuracy of mammographic diagnosis during screening depends on:
- Using optimal equipment to produce the mammogram. The routine use of AI enhances our detection by increasing our level of suspicion.
- The optimal image and reading are produced by a radiographer specialising in mammography.
- The optimal interpretation of the image is usually provided by doctors who specialise in mammography interpretation and read at least 2000 mammograms per year.
- A process of rigorous quality control, where all outcomes are recorded and regularly analysed.
Only where all these conditions are met will it be possible to realise the promise of lowering mortality rates from breast cancer and increasing breast conservation rates.
aging will detect about 95% of all breast cancers. Breast cancers that do not image are rare if the above criteria of a breast imaging centre are met. In such centres, women whose breast cancer is detected at screening will have the same survival chances as women without breast cancer.
With Automated Breast Volume Scanning (ABVS), which is 3D, the probe is moved automatically at a constant speed over the breast while images are constantly recorded. Post-acquisition image manipulation is possible with ABVS – such as three-dimensional reconstructions and rotations. Checking of images of the entire breast can be performed at a later stage as image acquisition and interpretations are separated, enabling review of images by several readers. These features greatly enhance the detection of small lesions especially in dense breasts.
In the case of breast cancer though it has been proven that certain factors do play a role in the risk of developing breast cancer. If these factors are present, you are at higher risk for developing breast cancer;
- Age (older)
- Being female
- Age at first childbirth (older)
- Age at first period (younger)
- Age at menopause (older)
- Alcohol consumption
- Ashkenazi Jewish heritage
- Body weight (heavier)
- BRCA1 or BRCA2 gene mutation
- Other genetic mutations predisposing to developing breast cancer e.g ATM, BARD1, BRIP1, CASP8, CTLA4, CYP19A1, FGFR2, H19, LSP1, MAP3K1, MRE11A, NBN, RAD51.
- Breast density (high)
- Family history of breast cancer
- Hyperplasia (benign breast condition)
- Lobular carcinoma in situ (LCIS)
- HRT
- Personal history of cancer
- Radiation exposure from medical imaging
- Radiation treatment during youth
- One or more women in your family were diagnosed with breast cancer at age 45 years or younger.
- Family history of cancers, such as prostate cancer, melanoma, and pancreatic cancer.
- There are breast and/or ovarian cancers in multiple generations on the same side of the family.
- A female relative is diagnosed with a second breast cancer in the same or the other breast or has both breast and ovarian cancers.
- A male relative is diagnosed with breast cancer.
- There is a history of breast and/or ovarian, pancreatic, or male breast cancer in a family of Ashkenazi Jewish ancestry.
- If you are at high genetic risk for breast cancer or already proven to be a carrier of a disease-causing mutation in the BRCA, ATM, CHEK or other high-risk genes, an MRI is indicated once a year. Please discuss this with your doctor at our multidisciplinary health care centre.
- Younger patients with dense breasts where it is difficult to identify the cancer on mammography may benefit from MRI evaluation to fully evaluate the extent of disease in the affected breast and exclude disease in the contralateral breast.
- In certain cases where the patient has DCIS- to better determine the extent of the disease.
With the newer technology that is available, minimal compression is required. Pain is now a thing of the past and at most, only women with very sensitive breasts may experience slight discomfort.
We also perform our imaging in a tranquil environment as we understand that it is also important for the patient to relax. When relaxed, the pectoral muscles behind the breast relax, which should result in a painless mammogram.
Breasts are usually the least sensitive at about 2 weeks after menstruation starts, so this may be the best time of the month to schedule a mammogram if this is a concern.
No. For over 40 years, millions of women have undergone mammography. As with all radiography, it involves exposure to X-Rays, but the dosage levels used are very low.
Mammographic techniques have also improved greatly over the past years. Currently employed techniques use only 0,1 to 0,2 rads per X-ray, which is an extremely low dose of radiation. This is equated to the cosmic radiation of about 30 minutes of air travel.
The question has also been asked as to whether compression can cause breast cancer. The answer is that compression doesn’t affect the breast tissue at all. For a useful mammogram, it is essential that the breast be compressed as the breast tissue needs to be spread out to allow breast structures to be seen.With appropriate compression the X-ray dose required can be reduced.
None of the above has been proven by science to cause breast cancer
Below is an infographic to visually give you a step-by-step guide on how to examine your breasts.
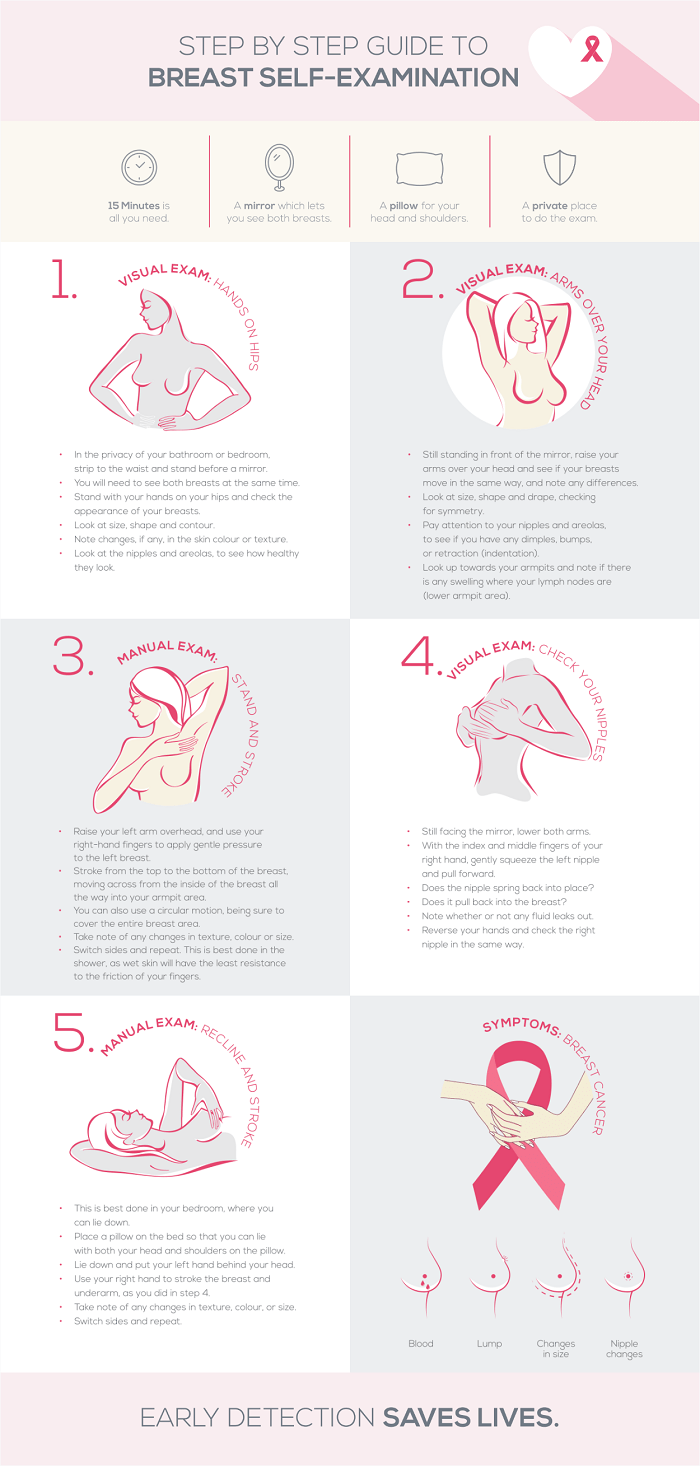
View our infographic page for larger version by clicking here.
Breast pain is usually due to hormonal influences on the breasts. During the menstrual cycle, the breasts are being prepared for pregnancy and subsequent breastfeeding in the same way that the womb is being prepared. The amount of fluid that is normally found in the breasts increases in volume (thus the milk glands and ducts literally swell up) up until menstruation when the hormone levels change and the fluid gets reabsorbed again. Breast tissue is not static and as we get older the breast tissue is replaced by fatty tissue. This process starts around 40 years of age but varies significantly between women. It causes a degree of fluid imbalance in the breast which may lead to new symptoms of breast tenderness or worsening of old symptoms. We call this process involution.
It is always good to have a thorough breast examination if any new breast symptoms arise. If no abnormality is found upon such a review, one of the following may be tried (try one at a time giving 4-6 weeks to monitor effect; 1-3 NOT recommended during pregnancy):
- Evening Primrose Oil 1-2grams 3 times per day.
- Mastodyn 2 tabs 3 times per day.
- Kelp 2 tabs 3 times per day (not to be used if you use thyroid medication or are being monitored for your thyroid).
- Low fat, no refined carbohydrates, high fibre diet.
- Minimise caffeine intake – bearing in mind green tea also contains caffeine.
Before having cosmetic breast surgery, it is recommended that you go for breast cancer screening. Any surgery to the breasts will make future evaluation of the breasts more complicated and can increase the chances of missing an existing cancer.
Yes. Breast augmentation does not constitute an increase in glandular tissue, so you are not more at risk. It is however necessary that an experienced mammographer does your mammogram, as special techniques are needed to demonstrate all breast tissue.
Good mammographic technique is of cardinal importance in producing high quality mammography.
A mammogram should only be mildly uncomfortable. However, if you are concerned about the tenderness of your breasts, it is advised that you see a trained breast health physician. In this instance, a clinical evaluation and an ultrasound can be performed. If anything suspicious is detected, an immediate mammogram may be required.
It is important to note that an ultrasound does not replace a mammogram, which remains the best tool for the diagnosis of breast cancer.
2-3 grams of Evening Primrose Oil per day for 2-4 weeks is noted to reduce breast tenderness.
Breasts are very resistant to injuries and an injury to the breast cannot cause breast cancer. Severe trauma can cause fat necrosis when tissue dies off. This is felt as a lump and can at times be mistaken for cancer on a mammogram. Fat necrosis is not a form of cancer and does not develop into cancer over time.
With regard to wine, alcohol and more importantly, its metabolite acetaldehyde, are highly carcinogenic, i.e. cancer-causing.
The good news, however, is that humans can metabolize both substances very effectively and therefore, when consumed in moderation, the cancer-causing effects of alcohol are barely noticeable. Wine, in particular, contains many bioactive substances known to decrease breast cancer risk and there is considerable evidence from in-vitro studies and observational studies, that moderate wine consumption as part of the “mediterranean” diet and lifestyle may reduce breast cancer risk.
Heavy alcohol use is universally accepted to be detrimental and greatly increases breast cancer risk and mortality.
- Lumps of any size or thickening of the breast tissue and or axillae.
- Any kind of skin change to the breast, areola or nipple area.
- Changes in the shape of the breast or persistent discomfort.
- Discharge from the nipple – that is not associated with pregnancy or breast-feeding.
Two approaches in combination have proven to be the most effective way of reducing breast cancer deaths: Screening mammography by specialised centres and treatment in a specialised, multidisciplinary centre, offering surgical, medical and radiation oncological as well as plastic surgical services by specialists in these disciplines that have a specific interest in breast health.
A case volume of more than 150 new cases of breast cancer per year has been shown to half the long-term recurrence rate.
Breast cancer metastasises to places outside of the breast. The tumour in the breast will not kill you – the spread of the cancer to the brain, lungs etc. will.
As breast cancer often spreads to other areas early in the course of the disease, a mastectomy will not guarantee you better survival than breast conserving therapy.
Should a mastectomy be necessary, breast reconstruction can often take place during the same session that the mastectomy is performed.
A multi-disciplinary treatment approach involves an oncologic surgeon, a radiation oncologist, a medical oncologist and a plastic surgeon who must optimally time and sequence the individual treatments.
In a well-run multidisciplinary breast clinic, out of 100 women with breast cancer approximately, 60 will have breast conserving therapy, 35 will have a mastectomy with immediate reconstruction and only 5 will leave the theatre with neither their own breast nor a reconstructed breast.
Immediate reconstruction has not been demonstrated to change recurrence rates, regardless of whether the reconstruction is prosthetic or with the patient’s own tissue.
A very important, but often overlooked factor is where a patient is treated.
It has been shown that depending on where the woman is treated for breast cancer, the risk of death within 5 years can be up to 60% higher in environments where only a few breast cancers are treated versus environments where more than 150 new breast cancer cases are treated per year.
A multidisciplinary team of specialists that have a specific interest in breast health, and who work with more than 150 new cases per year have been shown half the long-term recurrence rate.
The effect of a specialised and multidisciplinary treatment is greater than any chemotherapy, hormonal or radiation therapy.